
Calcium is one of the most critical minerals in the human body, essential for strong bones, nerve signaling, muscle contraction, and blood clotting. When calcium levels fall below normal—a condition known as hypocalcemia—it can trigger a cascade of health issues ranging from mild tingling to life-threatening complications. While many people assume calcium deficiency stems solely from poor diet, the reality is far more complex. Hypocalcemia often results from disruptions in hormonal regulation, organ function, or underlying medical conditions. Understanding the root causes is vital for accurate diagnosis and effective treatment.
The Role of Calcium and Its Regulation
Calcium isn't just about bone strength. About 99% of the body’s calcium is stored in bones and teeth, but the remaining 1% circulates in the blood and soft tissues, where it performs dynamic physiological functions. Blood calcium levels are tightly regulated by three key players: parathyroid hormone (PTH), vitamin D, and calcitonin.
Parathyroid hormone, released by the four small glands behind the thyroid, increases blood calcium by stimulating bone resorption, enhancing intestinal absorption via vitamin D activation, and reducing calcium excretion in the kidneys. Vitamin D, primarily obtained through sunlight exposure and diet, enables the gut to absorb calcium efficiently. When these systems fail—due to gland dysfunction, nutrient deficiency, or organ damage—calcium balance collapses.
“Hypocalcemia is rarely about dietary intake alone. It's usually a sign of deeper metabolic or endocrine disruption.” — Dr. Alan Reyes, Endocrinologist at Boston General Hospital
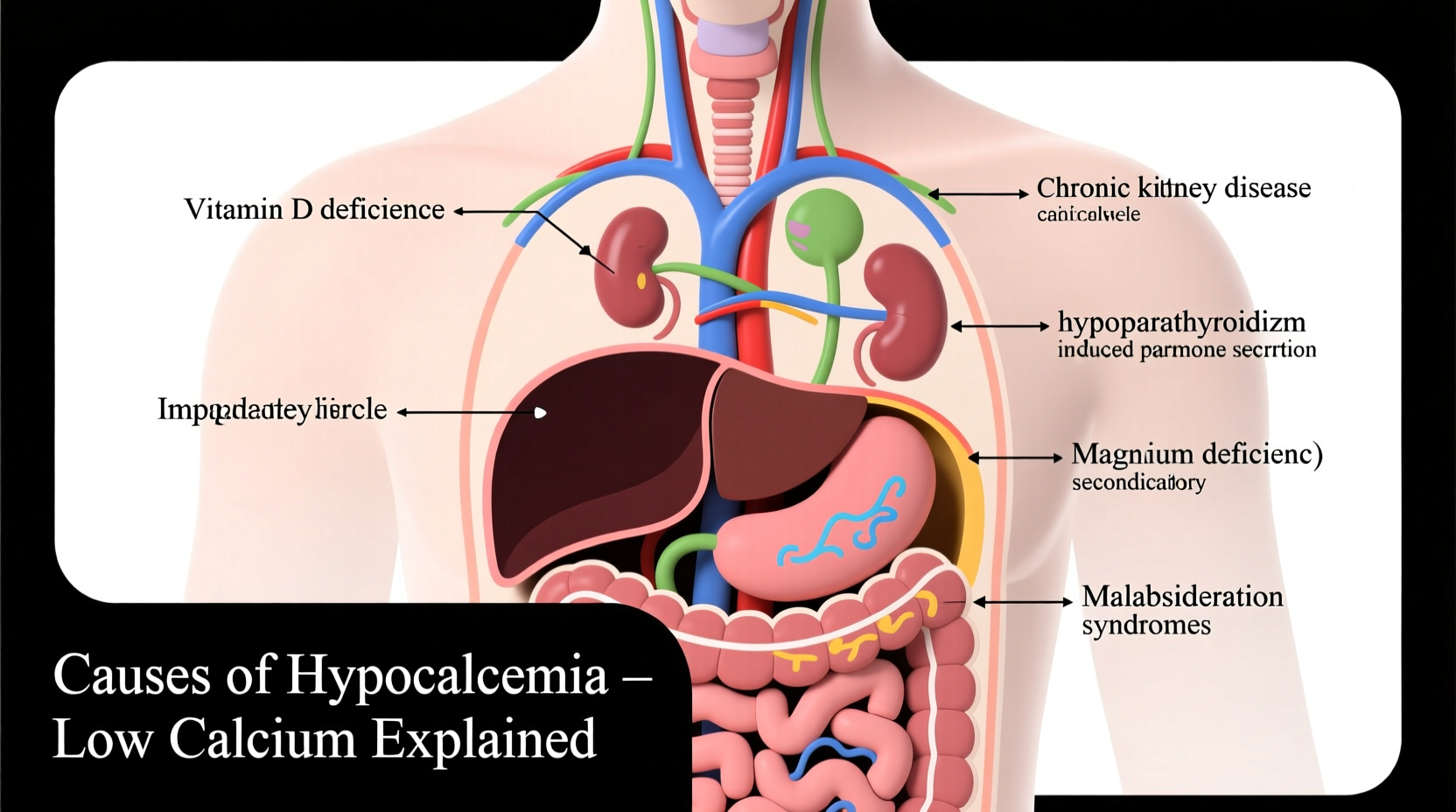
Common Causes of Low Calcium Levels
Hypocalcemia arises when calcium intake, absorption, or retention is compromised. The most frequent causes include:
- Chronic kidney disease: Impaired kidneys fail to activate vitamin D and excrete phosphate, leading to reduced calcium absorption and increased binding of calcium to phosphate.
- Hypoparathyroidism: Damage to or removal of parathyroid glands during neck surgery is the leading cause of permanent hypoparathyroidism, resulting in insufficient PTH production.
- Vitamin D deficiency: Limited sun exposure, malabsorption disorders (like celiac or Crohn’s disease), or inadequate dietary intake prevent proper calcium absorption.
- Magnesium deficiency: Magnesium is required for PTH secretion and action. Low magnesium impairs the body’s ability to respond to calcium needs.
- Acute pancreatitis: Inflammation triggers fat necrosis, which binds calcium and lowers serum levels.
- Medications: Certain drugs—including bisphosphonates, calcitonin, and some antiseizure medications—can interfere with calcium metabolism.
- Pseudohypoparathyroidism: A rare genetic disorder where tissues don’t respond to PTH, despite normal or elevated hormone levels.
Diagnosing Hypocalcemia: What Tests Reveal
Diagnosis begins with measuring serum calcium, but clinicians must interpret results carefully. Total calcium includes both bound (to proteins like albumin) and free (ionized) forms. Since only ionized calcium is biologically active, low albumin levels can falsely lower total calcium without true hypocalcemia.
To confirm the diagnosis, doctors assess:
- Ionized calcium level
- Parathyroid hormone (PTH)
- Vitamin D (25-hydroxyvitamin D)
- Magnesium and phosphate levels
- Renal function (creatinine, eGFR)
A low calcium with high PTH suggests compensation for deficiency—perhaps due to vitamin D lack or malabsorption. Conversely, low calcium with low or inappropriately normal PTH points to hypoparathyroidism. High phosphate alongside low calcium often indicates kidney failure.
Differential Diagnosis Table
| Cause | Serum Calcium | PTH Level | Vitamin D | Phosphate |
|---|---|---|---|---|
| Vitamin D Deficiency | Low | High | Low | Low/Normal |
| Hypoparathyroidism | Low | Low | Normal | High |
| Chronic Kidney Disease | Low | High (secondary hyperparathyroidism) | Low (inactive form) | High |
| Magnesium Deficiency | Low | Low/Normal (non-functional) | Variable | Low |
Recognizing Symptoms and When to Seek Help
Early signs of hypocalcemia are often subtle. Patients may experience:
- Numbness or tingling in fingers, toes, or around the mouth
- Muscle cramps or spasms, particularly in hands and feet (carpopedal spasm)
- Fatigue, anxiety, or irritability
- Brittle nails and dry skin
In severe cases, hypocalcemia can lead to seizures, arrhythmias, or laryngospasm. The Chvostek sign (twitching facial muscles when tapping the facial nerve) and Trousseau sign (hand spasm after inflating a blood pressure cuff) are clinical indicators used at the bedside.
“I started getting leg cramps at night after my thyroidectomy. I thought it was dehydration—turns out my calcium was dangerously low. My doctor caught it before things got worse.” — Maria T., patient case study
Managing and Preventing Hypocalcemia
Treatment depends on the underlying cause. Acute hypocalcemia with symptoms requires intravenous calcium gluconate under medical supervision. Chronic management focuses on correcting deficiencies and supporting regulatory systems.
Step-by-Step Management Plan
- Confirm diagnosis with ionized calcium and PTH testing.
- Check magnesium levels—correct deficiency first, as it blocks PTH response.
- Supplement vitamin D if deficient, typically with cholecalciferol (D3).
- Prescribe oral calcium (e.g., calcium carbonate or citrate), dosed throughout the day for better absorption.
- Monitor kidney function and phosphate levels regularly.
- Adjust diet to include calcium-rich foods: dairy, leafy greens, fortified plant milks, sardines, and tofu.
- Review medications that may contribute to calcium loss.
Prevention Checklist
- Get regular sunlight exposure (10–30 minutes several times a week)
- Eat calcium-rich foods daily
- Maintain adequate magnesium intake (nuts, seeds, whole grains)
- Have routine blood work if you have kidney disease or thyroid conditions
- Avoid excessive alcohol and smoking, which impair calcium metabolism
Frequently Asked Questions
Can low calcium cause long-term damage?
Yes. Chronic hypocalcemia can lead to cataracts, basal ganglia calcification, osteoporosis, and neurological decline if left untreated. Early intervention prevents complications.
Is dairy the only good source of calcium?
No. While dairy is rich in calcium, many non-dairy sources exist: collard greens, kale, bok choy, almonds, chia seeds, canned salmon with bones, and fortified cereals or plant-based milks.
Why do some people develop hypocalcemia after surgery?
Thyroid or parathyroid surgery can inadvertently damage or remove the parathyroid glands. This leads to postoperative hypoparathyroidism, affecting up to 30% of patients temporarily—and 1–5% permanently.
Conclusion: Taking Control of Your Calcium Health
Hypocalcemia is more than a simple nutrient shortfall—it's a signal that your body’s intricate mineral balancing system is under stress. Whether triggered by surgery, kidney dysfunction, or nutritional gaps, identifying the root cause is the first step toward recovery. With proper testing, targeted supplementation, and lifestyle adjustments, most people can restore and maintain healthy calcium levels. Don’t ignore persistent tingling, cramps, or fatigue. These may be early warnings worth investigating. Prioritize your metabolic health today to protect your bones, nerves, and heart tomorrow.








 浙公网安备
33010002000092号
浙公网安备
33010002000092号 浙B2-20120091-4
浙B2-20120091-4
Comments
No comments yet. Why don't you start the discussion?